Vestibular schwannoma
Vestibular schwannoma

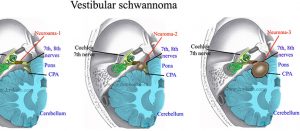
Vestibular schwannomas (VS) arise typically from the vestibular division of the eighth cranial nerve just within the internal auditory canal (IAC). It can be presented as a sporadic disease or in the spectrum of genetic disease like neurofibromatosis. As the VS grows, there is gradual compression of the fifth and seventh cranial nerves as well as the remaining divisions of the eighth cranial nerve; less often the ninth and tenth cranial nerves are compressed. As the tumor volume increases, the pons and lateral medulla are compressed with resultant initial effacement, and eventual obliteration, of the fourth ventricle and resultant obstructive hydrocephalus. The earliest and most frequently reported symptom is hearing loss. Because of the episodic nature, slow time course, and patient adaptation, it is not unusual for symptoms to be neglected for a long period of time prior to presentation. Patients will sometimes become aware of the inability to use a telephone on one ear, which will cause them to seek medical care.
Given the paramount importance of preserving neural function during surgery for VS, several techniques for intraoperative monitoring (IOM) of the relevant cranial nerves have been developed and refined over the past several years. The use of optimal monitoring techniques, along with the ability to correctly interpret and troubleshoot intraoperative signal changes, is critical for maximizing neural preservation.
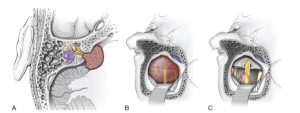
The retro sigmoid (RS) approach is used primarily for medium to large tumors. Often the most familiar approach to neurosurgeons, the RS approach affords an excellent view of the posterior cranial fossa contents, including the interface between the tumor and cerebellum/brainstem. Preservation of facial nerve function is an important consideration in VS surgery because facial paresis is associated with significant social implications. Preoperative tumor size has been shown to correlate with poorer facial nerve outcome postoperatively. Some patients suffer from incomplete facial palsy, which carries the main risk of morbidity to the eye. Immediate postoperative eye precautions should be instituted in order to prevent keratitis and corneal ulceration. The introduction of IOM and the ability to directly stimulate the facial nerve allow the surgeon to monitor, in real time, the structural and functional integrity of the nerve. This allows for early detection and the potential for prevention of an intraoperative injury, although once the signals are abnormal, neuromonitoring has limited ability to predict the extent of recovery.

{kind=link}
{kind=link}
{kind=link}